AC Joint Arthritis
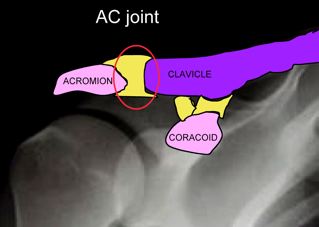
The acromioclavicular (AC) joint is the joint between the part of the shoulder blade known as the acromion and the collarbone (clavicle). The joint has a tendency to degenerate after 40 years of age but most arthritic AC joints are not painful. The most common form of arthritis is degenerative (osteoarthritis), but may also result from trauma, rheumatoid disease or infection. AC joint arthritis often occurs in association with other shoulder pathology such as impingement or rotator cuff tears.

AC joint pain is generally felt up on top or just in front of the AC joint. This is different from most rotator cuff pain that is felt down the deltoid muscle. AC joint pain is increased by:
- Sleeping on the effected shoulder
- Reaching across the front of your body at shoulder height
- Certain exercises such as bench press Patients who bench press to excess may develop a painful AC joint condition with erosion of the end of the collarbone (distal clavicular osteolysis)
Investigations that assist with the diagnosis include:
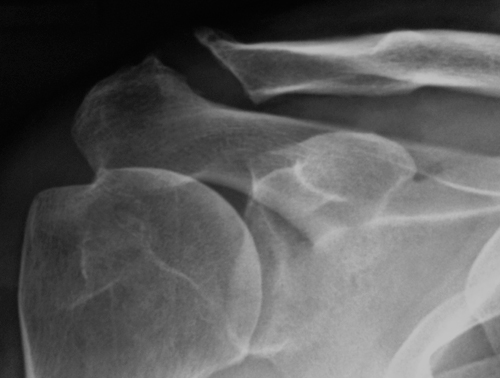
- X-rays: show loss of joint space, increased bone density and spurs either side of the joint
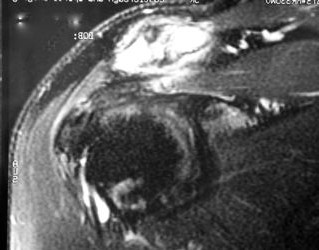
- MRI scans: show joint destruction and abnormal fluid in the bones either side of the joint
Non-operative treatment of AC joint arthritis is limited to activity modification and pain management. Strength exercises across a painful inflamed joint often aggravate symptoms. Pain management alternatives include simple pain killers, anti-inflammatories and corticosteroid injection. The corticosteroid injection can be helpful in confirming the diagnosis if it provides substantial relief. Unfortunately the relief from the injection is limited to a few weeks.
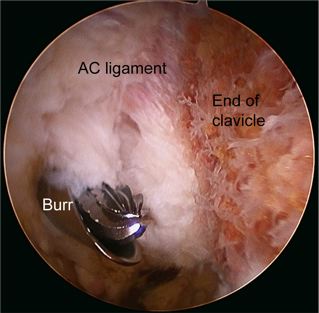
The operative treatment of AC joint arthritis is to remove the last 8mm of the collarbone (distal clavicular excision). This prevents the painful damaged joint surfaces from touching. This is performed by open or keyhole techniques. The procedure aims to not effect joint stability by preserving as much local ligament as possible. The procedure in isolation takes less than 1 hour and can be performed as a day stay or overnight procedure. Operation specific risks include but are not limited to infection, skin nerve injury and shoulder stiffness. Post-operatively a sling may be required for comfort only and range of motion exercises are commenced immediately. Pain-killers and anti-inflammatories may be required for several weeks. If performed in combination with other procedures such as a rotator cuff repair sling immobilisation will be greater to protect the other repair.