Shoulder Impingement
What is the shoulder?
The shoulder is a complex ball-and-socket joint that allows full movement of the arm.
It offers a wide range of motion, that also makes it vulnerable to injury.
At the shoulder, three major bones meet and create a 90-degree angle. These bones are the
- collarbone (clavicle)
- the shoulder blade (scapula)
- humerus, the largest bone of the arm.
Three joints are formed from the junctions of these three bones and the sternum. These joints are the
- glenohumeral joint,
- acromioclavicular (AC) joint and
- sternoclavicular joint.
Each joint in the shoulder is surrounded by cartilage for padding, ligaments to connect the bones, muscles and tendons to attach the muscles to the bones.
What is Shoulder Impingement?
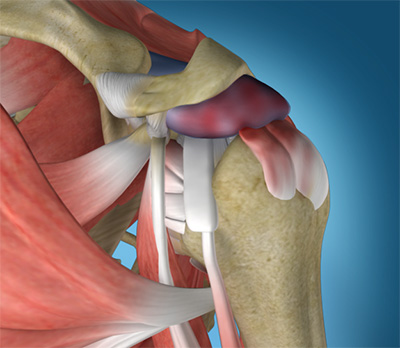
Shoulder Impingement is the painful catching of the tendon or bursa that occurs in the space between the head of the humerus and the shoulder blade arch (acromion).
Over time, Shoulder Impingement can lead to inflammation of the bursa and damage to the rotator cuff tendons.
Causes of Shoulder Impingement
- Repetitive use of arms overhead
- Repetitive lifting away from the body.
- Result of an injury: falling onto outstretched hand or elbow
Shoulder Impingement symptoms
Shoulder Impingement may have the following symptoms:
- Pain, present with activity and/or rest
- Pain radiating from the front of the shoulder to the side of the arm
- Pain with lifting and reaching movements (painful arc)
- Pain at night
- Loss of strength and motion
Diagnosis of Shoulder Impingement
The diagnosis of impingement
Consultation - During this consultation [doctor] will:
- take a medical history, with emphasis on pain, sleep disturbance, loss of function and treatments.
- perform a physical examination, documenting range of motion, strength and shoulder impingement signs.
Imaging tests - In order to understand the state of the rotator cuff tendons, bursal inflammation or bone spur formation, imaging scans are required:
- X-rays - do not show tendons but may show changes in the shoulder blade shape (spur, increased curvature or tilt) that may narrow the tunnel over the rotator cuff tendons. X-rays also exclude arthritis of the ball and socket or collar bone / shoulder blade (AC) joint that can also cause shoulder pain.


- Ultrasound - can visualise the bursa and rotator cuff tendons, compare both shoulders and examine the tendons for impingement with arm elevation.
- MRI - can create detailed images of both bone and soft tissues. An MRI can show bursitis, tendon thickening or tear and tunnel narrowing due to bony or ligament prominence. MRI scans require laying down in a tunnel and may not be tolerated by people with claustrophobia.
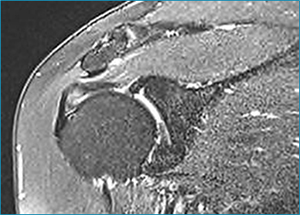
MRI scan showing pinching and damage to the tendon under the narrow tunnel.
While not all of these approaches or tests are required to confirm the diagnosis, this diagnostic process will also allow Dr Harper to review any possible risks or existing conditions that could interfere with the surgery or its outcome.
Treatment for Shoulder Impingement
When deciding on the appropriate treatment for Shoulder Impingement Dr Harper will consider you age, activity level and general health.
Nonsurgical Treatment:
- Activity Modification: avoiding tasks that exacerbate the pain.
- Pain Management: Analgesics, Non-steroidal anti-inflammatory medication and cortisone injections
- Physical therapy: with emphasis on restoring shoulder movement and strength.
Shoulder Impingement Surgery
Shoulder Impingement surgery may improve function and reduce pain to the shoulder joint. It may also reduce tendon damage and progression to tendon tear. Shoulder Impingement surgery was traditionally performed as open surgery, with long incisions, muscle detachment and a long recovery process.
Minimally Invasive Shoulder Surgery
Shoulder Impingement surgery can now be performed as a keyhole ( arthroscopic) procedure.Two or three small incisions (portals) are made. Each incision is called a portal.
In one portal, the arthroscope (camera) is inserted to view the shoulder joint. Along with the arthroscope, a sterile solution is pumped to the joint which expands the shoulder joint, giving the surgeon a clear view and room to work.
Images from the arthroscope are transmitted to a large television screen that allows the surgeon to assess the structures of the shoulder joint. The inflamed bursa is removed. The abnormal bone spur is removed with a high speed burr.


The integrity of the rotator cuff tendons is confirmed. Occasionally unexpected pathology such as a degenerate biceps tendon may be found that may require additional surgery.
Untreated Shoulder Impingement
Shoulder Impingement is not life threatening but can impact on a patient’s quality of life and function.
It can affect anyone: elite athletes and the active individual, manual labourers and office workers.
Shoulder Impingement can lead to
- Short Term: inflammation of the bursa and rotator cuff abrasion. .
- Long Term: rotator cuff tendons may thin, laminate and tear.
Impingement Surgery Risks
As with any major surgery there are potential risks involved. The decision to proceed with the surgery is made because the advantages of surgery outweigh the potential disadvantages.
It is important that the patient is informed of the risks before the surgery takes place.
Complications can be medical (general) or specific to arthroscopic acromioplasty surgery.
Medical complications include those of the anesthetic and your general well being. Almost any medical condition can occur so this list is not complete. Complications include:
- Allergic reactions to medications
- Heart attacks, strokes, kidney failure, pneumonia, bladder infections.
- Complications from nerve blocks such as infection or nerve damage.
- Blood Clots (Deep Venous Thrombosis) - Blood Clots can form in the arm muscles or legs and can travel to the lung (Pulmonary embolism). These can occasionally be serious and even life threatening. If the patient suffers arm pain, redness or swelling, or have shortness of breath at any stage, contact Dr Harper, your general practitioner or present to a local hospital.
Serious medical problems can lead to ongoing health concerns, prolonged hospitalisation or rarely death.
Specific complications for surgery are rare but may include:
Incomplete pain relief- the surgery usually reduces pain by 90% but this is not achieved in all cases.
Infection - Infections can occur superficially at the incision or in the joint space of the shoulder, a more serious infection. Infection rates are low for arthroscopic surgery ( ∠ 1%). If infection occurs it can be treated with antibiotics but may require further surgery.
Shoulder Stiffness - is a common complication that can be minimized with adequate pain management and compliance with your physiotherapy program prescribed by your surgeon.
Damage to nerves of Blood Vessels - Also rare but can lead to weakness or loss of sensation in part of the arm. Damage to blood vessels may require further surgery if bleeding is ongoing.
Surgery Preparation
If surgery is required, preparation is necessary to achieve the best results and recovery.
Preparing mentally and physically for surgery is an important step toward a successful result.
- Dr Harper will outline the treatment plan and
- patients will need to understand the process and their participation.
Performing a tailored exercise program before surgery (ie. pre-hab) with a physiotherapist may assist with surgical recovery.
Dr Harper will also need to:
- discuss any medications being taken, to see which ones should be stopped before surgery
- do not eat or drink anything, including water, for 6 hours before surgery
- stop taking aspirin, warfarin, anti-inflammatory medications or drugs that increase the risk of bleeding one week before surgery to minimise bleeding
- stop or cut down smoking to reduce your surgery risks and improve your recovery
Report any infections (dental, skin, chest, urinary) to Dr Harper prior to surgery as the procedure cannot be performed until all infections have cleared up.
Post Shoulder Impingement Surgery
The patient will wake up in the recovery room and then be transferred back to their hospital room.
- Pain medication will be provided to keep the patient comfortable.
- A bandage will be around the operated shoulder and the arm will be in a sling or brace.
- The sling will be worn for comfort only, with emphasis on early restoration of movement.
Dr Harper will see the patient prior to discharge and explain the findings of the operation and what was done during Surgery.
- The bandage will usually be removed the morning after surgery and waterproof dressings applied by nursing staff to the arthroscopic portals.
- It is normal for the shoulder to swell after the surgery. Placing ice-packs on the shoulder will help to reduce swelling. Ice packs should be applied to the area for 20 min 3-4 times a day until swelling has reduced.
The patient should keep a pillow under their elbow while lying in bed.
- The patient will not be allowed to lift anything over your head or anything greater than 1 kilo for the first 4 weeks.
- 10-14 days after surgery Dr Harper will see the patient to monitor their progress and remove the sutures.
It is recommended that the patient not drive while wearing a sling for safety reasons.
The patient will be given specific instructions regarding activity and a rehabilitation program. A strengthening program starts 4 weeks after surgery. Return to manual labour on full duties normally takes 12-16 weeks.
Eating a healthy diet and not smoking will promote healing.




