Collarbone Fractures
What is a Collarbone?
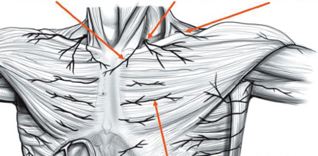
The clavicle, which is commonly known as the collarbone, is the bone found on both sides of the chest that connects the sternum or breastbone to both shoulders. It is the strut providing shoulder offset.
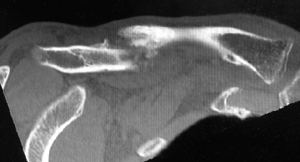
The clavicle sits above several important nerves and blood vessels.


What is a Collarbone Fracture?
A fractured clavicle is the medical term used when the collarbone is broken.
The clavicle is the most commonly fractured bone in the body. The principal cause of a broken collarbone is trauma (sports injuries, car accidents, falls). Rare causes include diseases that weaken the collarbone such as osteoporosis or cancer.
Collarbone fracture symptoms
Fractured collarbone sufferers have the following symptoms:
- Pain
- Sagging shoulder (down and forward)
- Inability to lift the arm because of pain
- A grinding sensation if an attempt is made to raise the arm
- A deformity or "bump" over the break
- Bruising, swelling, and tenderness over the collarbone
Diagnosis of Collarbone Fracture
Diagnosis is made with a consultation - During the consultation Dr Harper will:
- take a medical history : specifically assessing the amount of energy absorbed in the trauma. Commonly associated injuries such as scapula, rib fractures and/or haemothorax will be explored.
- perform a physical examination: looking for clavicular deformity, scapula asymmetry and bruising. Range of motion is limited and may be associated with crunching at the fracture site.
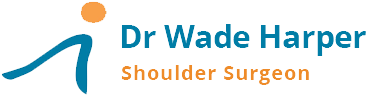
- Imaging tests -X-rays – an x-ray will define the break: the number of pieces and the degree of separation of the fragments. X-rays of the shoulder will be done to check for additional injuries (eg. scapula fracture).
While not all of these approaches or tests are required to confirm the diagnosis, this diagnostic process will also allow Dr Harper to review any possible risks or existing conditions that could interfere with the fracture management or its outcome.
Treatment for Collarbone Fracture.
If the broken ends of the bones have not shifted out of place and line up correctly, the patient is treated non-operatively. Broken collarbones have a high healing rate without surgery. If the patient’s bones are displaced, surgery may be appropriate to align the bones and hold them in position while they heal. This can improve shoulder function after recovery.
Non Surgical Treatment can include:
- Arm support
- Medication
- Physical Therapy

The patient will need to see your doctor until the fracture heals. The fracture can move out of place before it heals. If the bone heals in the wrong position, called a “malunion”, it can affect the patient’s shoulder function..
Collarbone Fracture Surgery
Plates and screws can be used to reposition and hold the bones into their normal alignment. The anatomic S shaped metal plates are applied to the upper surface of the bone.



Non-Operative treatment of Collarbone Fracture Risks
A Collarbone Fracture is not life threatening but can impact a patient’s quality of life and function.
Collarbone Fractures can lead in the
- Short Term - to pain, sleep disturbance and disability.
- Long Term - to malunion or non-union, that can result in ongoing pain and loss of function .
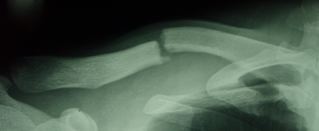
CT scan showing non-union of the clavicle.
Surgery Risks
As with any major surgery there are potential risks involved. The decision to proceed with the surgery is made because the advantages of surgery outweigh the potential disadvantages.
It is important that the patient is informed of these risks before the surgery takes place.
Complications can be general or specific to collarbone fracture surgery.
General complications include those of the anesthetic and your general well being. Almost any medical condition can occur so this list is not complete. Complications include:
- Allergic reactions to medications or anaesthetic.
- Complications from nerve blocks are rare but can include nerve damage that usually resolves.
- Blood Clots (Deep Venous Thrombosis) - occur very rarely after shoulder surgery. Blood clots can form in the arm or leg muscles and can travel to the lung (Pulmonary embolism). These can occasionally be serious and even life threatening. If the patient suffers arm pain, redness or swelling, or have shortness of breath at any stage, contact Dr Harper, your GP or your local hospital.
Serious medical problems can lead to ongoing health concerns, prolonged hospitalisation or rarely death.
Specific complications for surgery are rare but may include:
- Infection - Infections can occur superficially at the incision or deep and involve the plate. Infection rates for clavicle surgery are < 1% in healthy individuals. Infection can be treated with antibiotics but may require further surgery.
- Shoulder Stiffness - Shoulder stiffness with loss of range of motion is a common complication that can be minimized with adequate analgesia and adherence to your therapy program prescribed by your surgeon.
- Damage to nerves of Blood Vessels - The surgical incision required to insert a plate divides some small skin nerves over the front of the shoulder causing a numb patch that improves over 18 months but may never reach the same sensitivity as the non-operated side. It is very rare to injure a nerve that can lead to weakness or loss of movement in part of the arm. Damage to blood vessels may require further surgery if bleeding is ongoing.
Preparation for Collar Bone Surgery
If surgery is selected as the treatment of choice, preparation is necessary to achieve the best results and recovery.
Preparing mentally and physically for surgery is an important step toward a successful result.
- Dr Harper will outline the treatment plan and
- patients will need to understand the process and their participation.
Dr Harper will also discuss:
- any medications being taken, to see which ones should be stopped before surgery
- fasting times: do not eat or drink anything, including water, for 6 hours before surgery
- stop taking aspirin, warfarin, anti-inflammatory medications or drugs that increase the risk of bleeding one week before surgery to minimise bleeding
- stop or cut down smoking to reduce your surgery risks and improve your recovery
Report any infections (dental, skin, chest, urinary) to Dr Harper prior to surgery as the procedure cannot be performed until all infections have cleared up.
Post Surgery
The patient will wake up in the recovery room and then be transferred back to their hospital room after about 45minutes.
- Pain medication will be provided to keep the patient comfortable.
- A bandage will be around the operated shoulder and the arm will be in a sling or brace.
- The sling will be worn for comfort only.
Dr Harper will see the patient prior to discharge and explain the findings of the operation and what was done during surgery.
- The bandage will usually be removed before discharge and waterproof dressings applied.
- It is normal for the shoulder to swell after the surgery. Placing Ice-Packs on the shoulder will help to reduce swelling. Ice packs should be applied to the area for 20 min 3-4 times a day until swelling has reduced.
The patient should keep a pillow under their elbow while lying in bed.
- The patient will not be allowed to lift anything over your head or anything greater than 1 kilo for the first 6 weeks.
- 10- 14 days after surgery Dr Harper will see the patient to monitor their progress and remove the sutures.
It is recommended that the patient not drive while wearing a sling due to safety reasons.
The patient will be given specific instructions regarding activity and a rehabilitation program of exercise and strengthening.
Eating a healthy diet and not smoking will promote healing.




