Shoulder (Proximal Humeral) Fractures
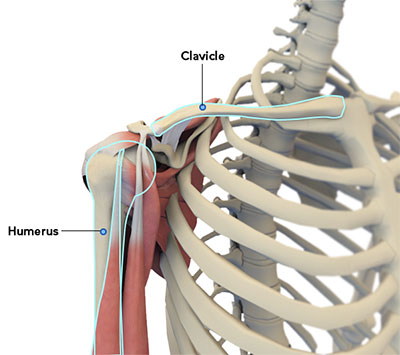
The shoulder joint is a ball and socket joint. A 'ball' at the top of the upper arm bone (the humerus) fits neatly into a 'socket', called the glenoid, which is part of the shoulder blade (scapula).
A fracture is a break in the bone that commonly occurs as a result of injury, such as a fall or a direct blow to the shoulder. A fracture of the upper part of the arm (proximal humerus) is more common in elderly individuals with osteoporosis. In younger individuals high energy trauma is generally required to cause these fractures.
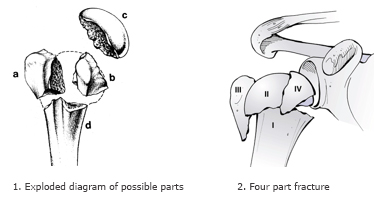
Proximal humerus fractures can be categorized into 4 groups:
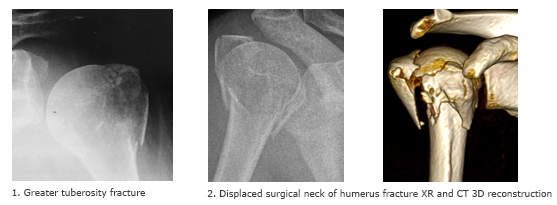
• Greater tuberosity fractures: Greater tuberosity is the insertion site for attachment of rotator cuff tendons. Greater tuberosity fractures are less common and are seen in cases of shoulder dislocations and in those with osteoporosis.
• Surgical neck fractures: Fractures of the surgical neck are most common in patients with osteoporotic bone.
• Lesser tuberosity fractures: These fractures are rare. If left untreated, these fractures cause loss of subscapularis muscle function ( a stabilizer and mobilizer muscle).
• Humeral head fractures: Humeral head fractures are rare..
Another way of describing proximal humerus fractures is by counting the number of displaced fracture fragments (two, three, and four part fractures) The more fragmentation of the proximal humerus, the higher risk of long-term loss of blood supply to the bone supporting the humeral head (avascular necrosis).
Patients with proximal humerus fractures experience pain, sleep disturbance, swelling, and restricted motion of the shoulder. Bruising may extend across the chest wall and down the arm.
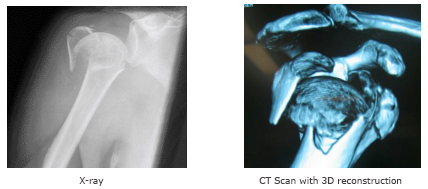
Proximal humerus fractures are diagnosed by history, physical examination and imaging of the affected area ( X-ray and/or computerized tomography (CT) scan).
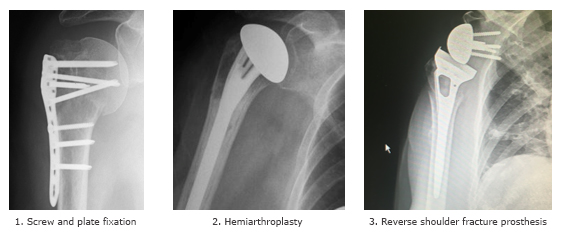
Most proximal humerus fractures are minimally displaced and can be treated non-operatively. This involves use of a sling to immobilize the arm and later physical therapy to restore function. Surgery may be necessary in displaced fractures. The multiple fragments are fixed with plates, screws, or a joint replacement.
Regardless of the form of treatment, stiffness (frozen shoulder) after a fractured neck of humerus, is very common. A course of physiotherapy is usually required to assist in regaining a functional range of motion. Maximal range of motion is achieved 12-18 months post fracture +/- surgery.
Other complications from surgical neck of humerus fractures include long-term pain, weakness and loss of function. Collapse of the humeral head due to a disrupted blood supply is delayed and rare but may require surgery to replace the fragmented joint surface. With surgery there are the additional risks associated with a general anaesthesia (often in the elderly), infection, nerve injury and greater stiffness.
Following fracture +/- surgery patients are encouraged to maintain sling immobilization and elbow range of motion. From 3 weeks post surgery, after surgeon review, the sling can normally be discarded and gentle range of motion exercises commenced. Patients can be active at waist level with their elbow against their side, lifting no more than 1L of milk.
3 weeks exercises: Lifting with normal arm.
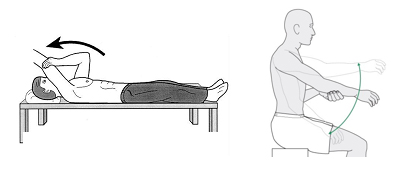
4 weeks exercises: Active assisted exercises
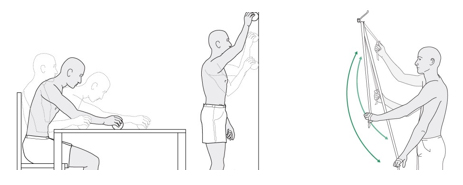
6 weeks: active elevation

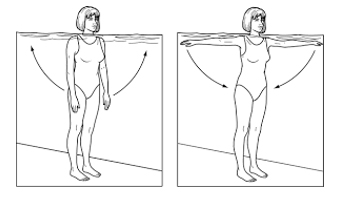
8 - 10 weeks: Strength/ hydrotherapy exercises
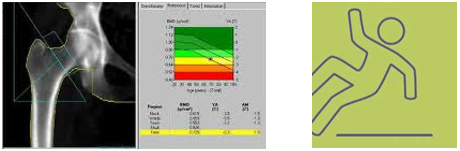
A low energy fall that results in a fractured neck of humerus may be an osteoporotic fracture. On recovery from this fracture it is recommended you have your bone mineral density assessed with your general practitioner. If you had previous borderline osteoporosis the fracture may make you eligible for treatments that reduce fracture risk. If you have had increasing falls, then a combined bone density and falls assessment clinic is recommended.