Rotator Cuff Tear
What is a Rotator Cuff?
The rotator cuff is made up of four muscles and their tendons that help move and stabilize the shoulder joint.
The four rotator cuff muscles include the:
- supraspinatus
- infraspinatus
- subscapularis
- teres minor
What is a Rotator Cuff Tear?
A rotator cuff tear is detachment of the tendon that attaches the muscle from the shoulder blade to the head of the humerus. Most tears occur in the supraspinatus tendon, however other areas of the rotator cuff may also be involved. It is common for these tendons to tear as people get older. Greater than 50% of people over 70 years of age have a full thickness tear at autopsy.
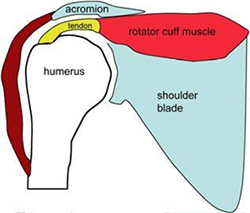
a. Tendon firmly attached to bone
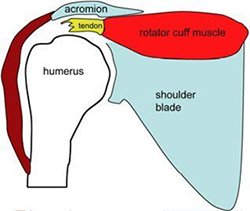
b. Tendon torn from bone bone
The tendon tear usually begins in a degenerate tendon that may fray and split. As the tendon damage progresses the tendon can tear.
There are different types of tears:
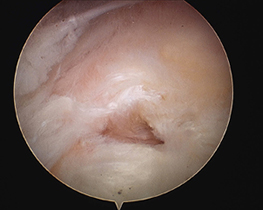
- Partial tear; some of the tendon attachment has ruptured but some fibres remain attached to the bone.
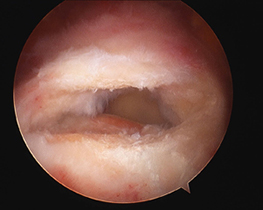
- Full-Thickness Tears; when the tendon is no longer connected to the bone.
Causes of Rotator Cuff Tear:
- Injury
- Degeneration
- Repetitive stress
- Lack of blood supply
- Bone spurs
- Or a combination of these factors
Rotator Cuff Tear symptoms
Rotator Cuff Tears can cause the following symptoms:
- Difficulty sleeping due to pain
- Difficulty lifting objects away from the body or overhead
- Weakness of the arm
- Crackling sensation when moving the patient’s shoulder (crepitus)
Diagnosis of Rotator Cuff Tear
Diagnostic methods include:
Consulation - During the consultation Dr Harper will:
- take a medical history: with emphasis on pain, loss of function and treatment.
- perform a physical examination, looking for tenderness, a painful arc, shoulder weakness and impingement signs.
Imaging tests - In order to clearly understand the rotator cuff pathology, imaging scans are required:
- X-rays - do not show tendons but may show changes in the shoulder blade shape (spur, increased curvature or tilt) that narrow the tunnel over the rotator cuff tendons and predispose to tears. X-rays also exclude arthritis of the ball and socket or collar bone / shoulder blade (AC) joint that can also cause shoulder pain.


X-rays showing acromial spurs.
- Ultrasound - can visualise the bursa and rotator cuff tendons, compare both shoulders and examine the tendons for impingement with arm elevation. Ultrasound can visualise shoulder tendons during movement of the arm.
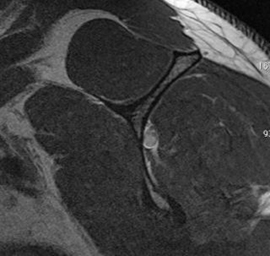
- MRI - can create detailed images of both bone and soft tissues. An MRI can show bursitis, tendon thickening or tear, muscle wasting and tunnel narrowing due to bony or ligament prominence. MRI scans require laying down in a tunnel and may not be tolerated by people with claustrophobia.
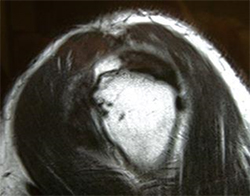

MRI scan: showing full thickness, full width tear of the supraspinatus tendon.
While not all of these approaches or tests are required to confirm the diagnosis, this diagnostic process will also allow Dr Harper to review any possible risks or existing conditions that could interfere with the surgery or its outcome.
Treatment for Rotator Cuff Tear
Non Surgical Treatment includes:
- Activity Modification: avoiding tasks that exacerbate the pain
- Pain Management: Analgesics, non-steroidal anti-inflammatory medication and cortisone injections
- Physical therapy: with emphasis on restoring shoulder movement and strength.
Arthroscopic Rotator Cuff Tear Surgery
If despite an ideal non-operative program, the patient still has pain and disability that interferes with their quality of life, then surgical options can be considered. For acute large traumatic tears in younger patients, surgery may be considered early.
Arthroscopic rotator cuff surgery is performed using a combination of an arm anaesthetic block and general anaesthesia. The local anaesthesia arm block is placed in the neck using ultrasound visualisation and numbs the affected shoulder and the arm for 12-24 hours.
- Multiple small incisions (portals) are made around the shoulder to view, manipulate and fix the rotator cuff tendons. The arthroscope is inserted through different portals to view the shoulder joint from different angles..
- A sterile solution is pumped to the joint which expands the shoulder joint, giving the surgeon a clear view and room to work.
- The magnified image on the television screen allows the surgeon to see the joint structures, determine the extent of the injuries and perform the surgical procedure.
- The glenohumeral joint is inspected first, documenting the state of the long head of biceps tendon, subscapularis tendon and joint cartilage.
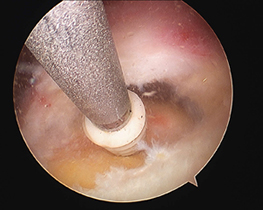
- The bursa and spur on the acromion are removed.
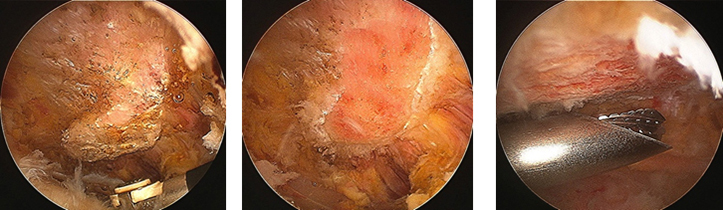
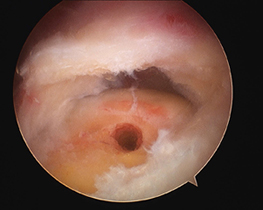
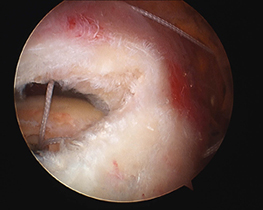
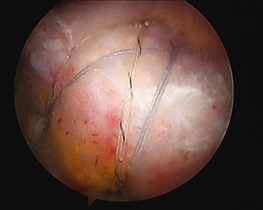
The rotator cuff tear is repaired
- small plastic anchors that are screwed into the humeral rotator cuff insertion. The anchors contain strong braided sutures or tapes that are placed through the torn rotator cuff tendons. Using knots or further anchors the tendons are attached back the bone of the humerus (arm).
Other pathology may need to be managed at the time of surgery to address other sources of pain and ensure a lasting result. These include:
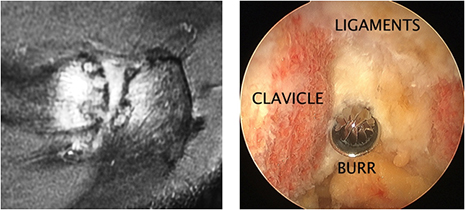
- An arthritic AC joint. An AC joint, that is clinically tender and arthritic on MRI can be a cause of incomplete pain relief after rotator cuff repair. The surgical management involves the removal of bone from both the clavicle and acromion to create an 8mm gap that prevents bone the painful bone ends making contact. The AC joint ligaments are preserved as much as possible to maintain AC joint stability.
- A degenerate, frayed, dislocating or inflamed long head of bicep tendonis is usually removed from the joint. This may be achieved by releasing the biceps from the socket and letting it retract into the bicipital groove (tenotomy) or by shortening the tendon and securing into the proximal humerus (tenodesis). Tenodesis is favoured in the more active patients as it restores muscle strength.
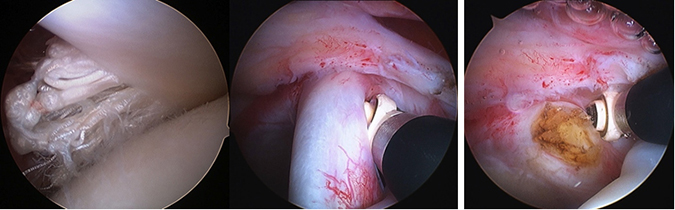
A damaged bicep tendon, being removed from the joint.
At the completion of surgery, the incisions (portals) are closed by sutures and the patient is taken to the recovery room in a sling.
Untreated Rotator Cuff Tear
A Rotator Cuff Tear is not life threatening but can impact on a patient’s quality of life, sleep and function.
The tear does not heal by itself and will gradually increase in size. The remaining attached muscles can be strengthened to help accommodate the tendon tear.
Rotator cuff tears can lead in the short term to pain, sleep disturbance, weakness and disability. In the long term, chronic large tears can lead to pain that can be difficult to control. There may be weakness performing tasks at arms length or overhead. If the tears are retracted a long way, the muscle belly has shrunk and lost fibres, the tears may become irreparable. Irreparable tears can progress to arthritis.
Normal muscle bellies on the shoulder blade

Loss of muscle with chronic tendon tears
Rotator Cuff Surgery Risks
As with any major surgery there are potential risks involved. The decision to proceed with the surgery is made because the advantages of surgery outweigh the potential disadvantages.
It is important that the patient is informed of these risks before the surgery takes place.
Complications can be general or specific to rotator cuff surgery.
General complications include those of the anesthetic and your general well being. Almost any medical condition can occur so this list is not complete. Complications include:
- Allergic reactions to medications
- Heart attacks, strokes, kidney failure, pneumonia, bladder infections.
- Complications from nerve blocks such as nerve damage.
- Blood Clots (Deep Venous Thrombosis)- Blood Clots can form in the arm or leg muscles and can travel to the lung (Pulmonary embolism). These can occasionally be serious and even life threatening. If the patient suffers arm pain, redness or swelling, or have shortness of breath at any stage, contact Dr Harper, your GP or local hospital.
Serious medical problems can lead to ongoing health concerns, prolonged hospitalisation or rarely death.
Specific complications for surgery are rare but may include:
- Infection- Infections can occur superficially at the incision or in the joint space of the shoulder, a more serious infection. Infection rates vary but are generally <1% and are higher in diabetes. If an infection occurs it can be treated with antibiotics but may require further surgery.
- Shoulder Stiffness- Shoulder stiffness is a common complication after all types of shoulder surgery. It is important to maximize pain management and comply with physiotherapy. If a post-operative frozen shoulder occurs it usually resolves by 9-12 months after surgery.
- Damage to superficial skin nerves can occur with incisions around the shoulder
- Incomplete Tendon Healing or retear. Despite the surgeon’s best efforts not all rotator cuff repairs will completely heal. Usually if there is a residual defect it is smaller than before surgery and this often provides similar pain relief. The tendon that is repaired is damaged, it does not heal in the same way as the original tendon insertion and requires long term modifications in activity to prevent re-tear.
Preparation Rotator Cuff Surgery
If surgery is required, preparation is necessary to achieve the best results and recovery.
Preparing mentally and physically for surgery is an important step toward a successful result.
- Dr Harper will outline the treatment plan and
- patients will need to understand the process and their participation.
Performing a tailored exercise program before surgery (ie. pre-hab) with a physiotherapist may assist with surgical recovery.
Dr Harper will also need to discuss:
- any medications being taken, to see which ones should be stopped before surgery
- fasting times: do not eat or drink anything, including water, for 6 hours before surgery
- stop taking aspirin, warfarin, anti-inflammatory medications or drugs that increase the risk of bleeding one week before surgery to minimise bleeding
- stop or cut down smoking to reduce your surgery risks and improve your recovery
Report any infections (dental, skin, chest, urinary) to Dr Harper prior to surgery as the procedure cannot be performed until all infections have cleared up.
Post Surgery
The patient will wake up in the recovery room and then be transferred back to their hospital room.
- Pain medication will be provided to keep the patient comfortable.
- A bandage will be around the operated shoulder and the arm will be in a sling or brace.
- The sling will be worn for 6 weeks to facilitate healing.

Dr Harper will see the patient prior to discharge and explain the findings of the operation and what was done during surgery.
- The bandage will usually be removed the morning after surgery and waterproof dressings applied. If the dressings remain clean, these can be left on until suture removal 10-14 days post surgery..
- It is normal for the shoulder to swell after the surgery. Placing Ice-Packs on the shoulder will help to reduce swelling. Ice packs should be applied to the area for 20 min 3-4 times a day until swelling has reduced.
The patient should keep a pillow under their elbow while lying in bed.
- During the first 6 weeks, while in the sling, light objects ( up to a can of drink) can be held or stabilised in the operated arm .
- It is recommended that the patient not drive during the first 6 weeks while wearing a sling due to safety reasons and the risk of injury to the surgical site.
- 10- 14 days after surgery Dr Harper will see the patient to monitor their progress and remove the sutures.
- It takes 12 weeks to establish healing with fibres that connect the tendon to bone.The patient will not be allowed to reach, lift the arm over head or perform any resistance / strength exercises until 12 weeks after the surgery.
6-12 Weeks Post Rotator Cuff Repair
- Sling can be removed. Reapplied for short periods only if pain. No sling after 8 weeks post surgery
- Can be active at waist level with elbow by side. No lifting more than 1kg in daily activities
- All 4 exercises 3 times per day, 10-20 repetitions per exercise
1. Shoulder Blade Exercises
- Elevation / depression
- Retraction (pictured) / protraction

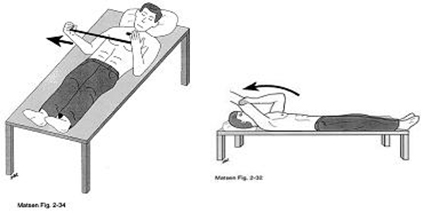
2. Desk Slide Exercises: both hands are placed o a book and the non-operated shoulder slides the book forward and backward to stretch the operated shoulder.

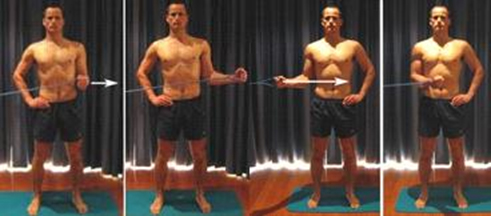
3. External Rotation Exercises: with elbow locked in by side of body. Can be active if no infraspinatus tendon repair
4. Passive Elevation Exercises lying down. Use good arm to lift operated arm. Do not bring arm all the way down until final repetition. Gradually increase range
> 12 Weeks Post Rotator Cuff Repair
- Active arm elevation can start, initially while laying down, in water or with bent elbow (decreased lever arm).
- A rubber band strengthening program can commence with the upper arm and elbow remaining close by the chest.
Eating a healthy diet and not smoking will promote healing.




