Shoulder Instability
What is the shoulder?
The shoulder is a complex ball-and-socket joint that allows excellent movement of the arm.
This wide range of motion makes the shoulder vulnerable to injury.
At the shoulder, three major bones meet and create a 90-degree angle. These bones are the collarbone (clavicle), the shoulder blade (scapula)—commonly known as the shoulder blade and the humerus.
Three joints are formed from the junctions of these three bones and the sternum. These joints are the glenohumeral joint, the acromioclavicular (AC) joint and the sternoclavicular joint.
Each joint in the shoulder is surrounded by cartilage for padding, ligaments to connect the bones and tendons to attach the muscles to the bones.
What is Shoulder Instability?
Shoulder instability is a condition where the ball can move excessively on the socket.
A dislocation occurs when the end of the humerus, the ball portion, slips off the socket portion of the shoulder. A partial dislocation is referred to as a subluxation whereas a complete separation is referred to as a dislocation.
Shoulder Instability increases the chance of further dislocation with every occurrence due to damage and stretching of the ligaments.
Causes of Shoulder Instability
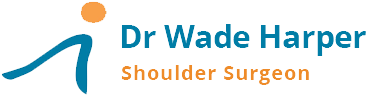
- Injury to the ligaments that normally stabilise the shoulder .The ligaments run from the neck of the ball to the socket. They are more like rope than rubber bands and generally have to tear to dislocate the shoulder.
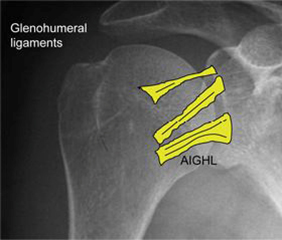

The ligaments attach to the socket via a cartilage ring called the labrum. If excessive force is placed on the arm, the ligaments can pull the labrum off the socket (Bankart Lesion). The ligament may not heal in its normal position, allowing increased movement of the ball on the socket that can predispose to further instability episodes.
- Generalised ligamentous laxity, commonly referred to as being double jointed.
- Large Rotator Cuff Tears
- Epilepsy and electrocution: can cause rarer posterior instability
Shoulder Instability symptoms
Shoulder Instability generally causes acute pain and sufferers have the following symptoms:
- Recurrent instability episodes or dislocations
- Pain during activities
- Pain at night and the following morning
- A sensation of the shoulder joint moving out of place
- Numbness or stingers in the arm on return to sport
Diagnosis of Shoulder Instability
Diagnosis of Shoulder Instability requires a history, examination and investigations.
Consultation - During this consultation Dr Harper will:
- take a medical history: with emphasis on the mechanism of injury, age of first dislocation, need for hospital reductions and disability
- perform a physical examination: looking at range of motion, strength, nerve injury and apprehension with arm positions
Imaging tests -
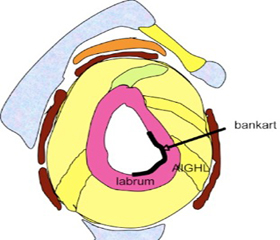
- X-rays – these pictures will show injuries to the bones that make up the shoulder joint. This may include a fracture of the socket (bony Bankart) or a crush fracture to the back of the humeral head (Hill-Sachs lesion)
- CT scan with 3D reconstruction - are used to accurately assess bone loss as a result of instability
Glenoid bone loss.

Hill-Sach's Lesion

Interaction of bone defects
- MRI - can create detailed images of both hard and soft tissues. The MRI scan can confirm the site of the ligament tear, cartilage damage, integrity of the rotator cuff tendons and fractures.
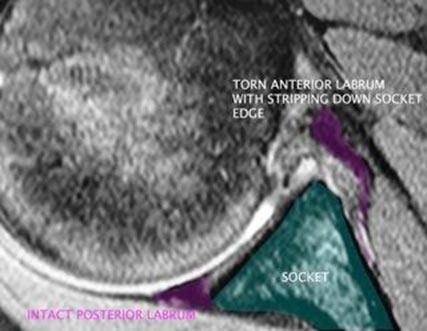
MRI scan.
- Examination under anaesthesia & Arthroscopy - In complex instability, despite the above investigations, the direction and extent of pathology may require an examination under anaesthesia and keyhole camera assessment of the joint.
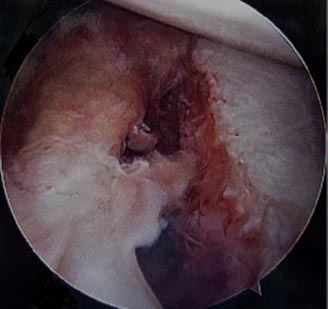
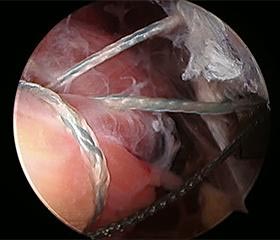
Anterior Translation Pre Repair
Arthroscopic image showing the cartilage rim (labrum) torn from the socket (bottom right)
While not all of these approaches or tests are required to confirm the diagnosis, this diagnostic process will also allow Dr Harper to review any possible risks or existing conditions that could interfere with the surgery or its outcome.
Shoulder Instability Treatments
Shoulder instability may be treated with nonsurgical or surgical options. If the nonsurgical options fail to restore shoulder stability and confidence, surgery may be needed.
Non Surgical Treatments:
- Immobilisation: slings can be worn for comfort. Prolonged immobilisation increases weakness and does not prevent recurrence
- Physical Therapy: can help restore range of motion and strength. This may be the principal therapy for “double jointed” patients with lax ligaments and no tears.
- Activity modification: patients who dislocate out the front have to avoid, in the long term, having their arm in the throwing position under load.
Shoulder Instability Surgery
Shoulder Stabilisation surgery may restore stability and function to the shoulder joint.
Shoulder stabilisation surgery has traditionally been performed as open surgery, with larger incisions and division of tendons for access. Open shoulder stabilisation may be required in certain cases and is my preferred method for patients with bone loss that requires bone grafting.
Minimally Invasive Shoulder Surgery
Shoulder Stabilisation surgery can also be performed arthroscopically, depending on the patient’s particular situation, with much smaller incisions. Rarely, arthroscopic surgery may need to be converted to open surgery to properly repair the damage to internal structures.
Three small incisions(portals) are made. Each incision is called a portal.
In one portal, the arthroscope is inserted to view the shoulder joint. Along with the arthroscope, a sterile solution is pumped to the joint which expands the shoulder joint, giving the surgeon a clear view and room to work.
The image from the arthroscope is magnified and projected onto a television screen. This allows the surgeon to assess the extent of the injuries and perform the necessary surgical procedure.
This may involve repairing a tear in the labrum as well as tightening the capsule and ligaments.
After stabilising the shoulder, the portals (incisions) are closed by suturing or by tape.
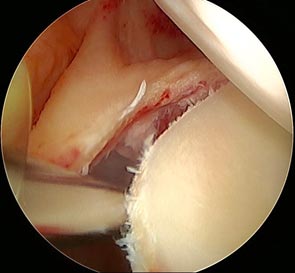
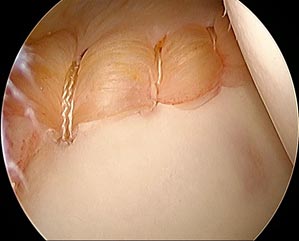
Arthroscpic images showing labral tear on left and labral repair on right
Remplissage Procedure
The remplissage procedure can be added to the arthroscopic Bankart repair to increase shoulder stability. The procedure is reserved for individuals who have a large crush fracture in the back of the humeral head ( Hill-Sach's lesion), with minimal bone loss on the socket. In the remplissage procedure, the fracture surface is freshened and anchors with sutures are used to tie the adjacent rotator cuff tendon into the defect. The humeral head, compressed bone defect is excluded from the joint and can no longer engage over the front of the socket.

Anchors are placed into the Hill-Sachs
Bone Deficient Anterior Instability
In shoulder instability there can be loss of bone on the socket, humeral head or both. The failure rate for arthroscopic labral repair in contact athletes with significant bone defects has been reported as high as 2/3. Addressing the bone defects with a glenoid bone graft reduces the recurrence of instability. My preferred technique is the Latarjet procedure. This technique fixes local coracoid bone graft with attached tendons to the anterior glenoid neck.


This is performed as an open procedure +/- arthroscopy. The procedure takes approximately 2 hours to perform. Most patients stay 1 night in hospital. This is also a salvage procedure for difficult instability cases.


X-rays showing screw fixation of the coracoid bone graft to the socket
Untreated Shoulder Instability
Shoulder Instability is not life threatening but can impact on a patient’s quality of life.
It can affect anyone: elite athletes, active individuals, manual labourers and office workers.
Recurrent instability can lead to
- Short Term Impact - ongoing pain, loss of confidence and restricted activity
- Long Term Impact - chronic instability can cause cartilage and bone loss that predispose to the early onset of shoulder arthritis

Arthroscopic image showing advanced cartilage loss with chronic instability
Shoulder Stabilisation Surgery Risks
As with any major surgery there are potential risks involved. The decision to proceed with the surgery is made because the advantages of surgery outweigh the potential disadvantages.
It is important that the patient is informed of these risks before the surgery takes place.
Complications can be general or specific to shoulder stabilization surgery.
Medical complications include those of the anesthetic and your general well being. Almost any medical condition can occur so this list is not complete. Complications include:
- Allergic reactions to medications, surgical skin preparations or dressings.
- Complications from nerve blocks such as infection or nerve damage.
- Blood Clots (Deep Venous Thrombosis) - Blood Clots can form in the arm muscles and can travel to the lung (Pulmonary embolism). This is exceedingly rare in the setting of shoulder stabilisation surgery. These clots can occasionally be serious and even life threatening. If the patient suffers arm pain, redness or swelling, or have shortness of breath at any stage, contact Dr Harper.
Serious medical problems can lead to ongoing health concerns, prolonged hospitalisation or rarely death.
Specific complications for surgery are rare but may include:
- Infection - Infections can occur superficially at the incision or in the joint space of the shoulder, a more serious infection. Infection rates vary but are generally <1%. If an infection occurs it can be treated with antibiotics but may require further surgery.
- Shoulder Stiffness - Shoulder stiffness is a common complication after shoulder surgery. There may be a slight loss of rotation with stabilisation surgery, usually less than 10 degrees in any plane. If stiffness is greater than expected, it usually recovers spontaneously over 8-12 months and may be improved with physiotherapy.
- Dislocations - Dislocations and/or subluxations with activity can occur on return to activity, if the force absorbed by the shoulder is greater than the strength of the repair. Recurrence rates after instability surgery are around 10 %.
- Damage to nerves of Blood Vessels - Also rare but can lead to weakness or loss of sensation in part of the arm. Nerve injury is higher with revision stabilisation and/or open surgery with bone grafts. Damage to blood vessels may require further surgery if bleeding is ongoing.
- Damage to the joint - Joint damage to the cartilage or other structures can rarely occur during surgery.
- Hemarthrosis - A condition caused by excess bleeding into the joint after the surgery is completed. This may require additional surgery to irrigate the joint.
Surgery Preparation
Once the decision to proceed to surgery has been made, preparation is necessary to achieve the best results and recovery.
Preparing mentally and physically for surgery is an important step toward a successful result.
- Dr harper will create a treatment plan
- patients will also need to understand the process and their role in the plan.
Participating and completing a tailored exercise program before (ie. pre-hab) with a trained physiotherapist may assist after surgery.
Dr Harper will also discuss:
- ceasing non-essential medications that may interfere with surgery.
- fasting times: do not eat or drink anything, including water, for 6 hours before surgery
- stop taking aspirin, warfarin, anti-inflammatory medications or drugs that increase the risk of bleeding one week before surgery to minimise bleeding
- stop or cut down smoking to reduce your surgery risks and improve your recovery
Report any infections to Dr Harper prior to surgery as the procedure cannot be performed until all infections have cleared up.
After Shoulder Stabilization Surgery
The patient will wake up in the recovery room and then be transferred back to their hospital room.
- Pain medication will be provided to keep the patient comfortable. This will usually include simple analgesics, an oral opiate medication and an anti-inflammatory tablet. These are usually required for 3-4 days after surgery.
- A bandage will be around the operated shoulder and the arm will be in a sling.The sling will be worn for about 6 weeks to facilitate healing.
Dr Harper will see the patient prior to discharge and explain the findings of the operation and what was done during Surgery.
- The bandage will usually be removed after surgery and waterproof dressings provided by your nurse over the area.
- It is normal for the shoulder to swell after the surgery. Placing Ice-Packs on the shoulder will help to reduce swelling. Ice packs should be applied to the area for 20 min 3-4 times a day until swelling has reduced.
The patient should keep a pillow under their elbow while lying in bed.
- The patient will not be allowed to lift anything greater than 1 litre of milk for the first 6 weeks.
- 10-14 days after surgery Dr Harper will see the patient to monitor their progress and remove the sutures.
It is recommended that the patient not drive during the first 6 weeks while wearing a sling due to safety reasons and the risk of injury to the surgical site.
The patient will be given specific instructions regarding activity and a rehabilitation program of exercise and strengthening.
Eating a healthy diet and not smoking will promote healing.




